CHAPTER 22
Spina Bifida
WHAT IS IT?

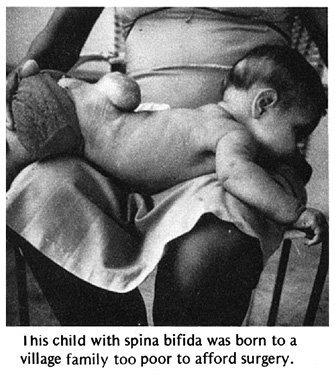
Spina bifida (also called meningocele or myelomeningocele) is a defect that comes from a problem in the very early development of the unborn child. It happens when some of the back bones (vertebrae) do not close over the center tube of nerves (spinal cord). As a result, a soft unprotected area is left, which may bulge through the skin as a dark bag. This 'bag of nerves' is covered by a very thin layer (membrane) which may leak liquid from the spinal cord and brain. Nobody knows what causes it. But 1 of every 250 to 500 babies is born with spina bifida.
Problems that occur with spina bifida
| High risk. Without early surgery to cover the
bag of nerves, it almost always gets infected and the child dies
of meningitis.
|

| Muscle weakness and loss of feeling. The legs or feet may be paralyzed and have little or no feeling. | |
| Hips. One or both hips may be dislocated. |

| The feet may turn down and in (club feet), or up and out. | |
| If the defect is relatively high up the back (L1 or above, see next page), there may be muscle spasms (spasticity) in the legs and feet (see Page 176). | |
| Poor urine and bowel control. The child may not feel when he pees or has a stool. When he gets older he may not develop control, and will pee or shit without knowing it. |

| Big head. 'Hydrocephalus', which means 'water on the brain', develops in 4 out of 5 children with spina bifida. The liquid that forms inside the head cannot drain normally into the spinal cord, so it collects and puts pressure on the brain and skull bones. Although the child's head may look normal at birth, little by little it becomes swollen with liquid, like this. | |
| very big head | |
| big veins | |
| The eyes may turn downward because of pressure in the head. This 'setting sun sign' means danger of blindness and severe brain damage. | |
| Brain damage. Without early surgery to lower the pressure of the liquid in the head (and sometimes even if the surgery is done), some children become blind, mentally retarded, have fits (epileptic seizures, see Page 233), or develop cerebral palsy (see Chapter 9). |
PROBLEMS THAT MAY OCCUR WHEN THE CHILD IS OLDER:

| Curve of the spine (See Chapter 20.) | |
| Urinary infections and kidney damage (See Page 210.) |

| Pressure sores may form over the bones, because the child cannot feel. (See Chapter 24.) |

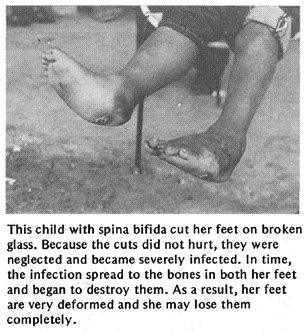
| Foot injuries. Children who can walk but have no feeling in their feet may easily develop sores or injuries. If neglected, these can lead to severe infections of the flesh, bone infection, and deformities or loss of the feet (see Page 222). |
What is the future for a child with spina bifida?
This will depend first on how serious the defect is, next on medical treatment and general care, and finally on special training and on family and community support.

The higher up the back the defect is or the more severely the spinal cord is affected, the worse the paralysis and other problems are likely to be. If the head is already very swollen, the child's chances are poor. The costs will usually be great, even for a rich family. Surgery to drain the liquid from the head is sometimes followed by infection. The operation may need to be repeated several times. In spite of the best medical attention, at least 1 of every 4 or 5 children born with severe spina bifida dies in the first months or years of life.
However, the child with a defect that is low down on the back usually has less paralysis, and has a good chance of living a full and happy life. With good family and community support, many children with spina bifida go to school, learn to do many kinds of work, get married, and have children.
Often these children are late in learning basic skills for self-care (getting dressed, eating, going to the bathroom). This is partly because of the disability. But it is also because their parents often overprotect them and do everything for them. It is important for parents to help these children to do more for themselves.
What are the chances that my child with spina bifida will walk?
This depends on many factors. However, the higher up the defect is on the spine, the more paralysis the child will probably have. The drawings below show how likely it is for the child to walk, based on the level of the defect. The shaded areas show the parts of the body affected by paralysis and loss of feeling.
|
PROBABLE AMOUNT OF DISABILITY
|
|||||

|
||||||

|

CARING FOR THE CHILD WITH SPINA BIFIDA
Care of the defect. When there is a 'bag of nerves' on the spine of a newborn baby, his chances of living are much better if he has an operation within a few weeks. The surgery covers the defect with muscle and skin. Without this operation there is a high risk of injury and brain infection (meningitis); the child will probably not live very long.
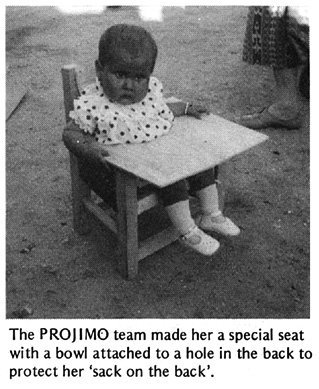
For children who cannot get an operation, try to protect the bag of nerves so that its thin covering is not injured or broken. (if it breaks, meningitis can occur.)
One way to protect the bag is to make a ring or 'donut' of soft cloth or foam rubber, and to tie it so that it surrounds the bag. Do not let the ring or clothing touch the bag.

|

|

|

|
Hydrocephalus. It is important to measure the distance around the head of the child at birth, and every week or so afterward. If head size increases faster than normal (see chart on Page 41), or if you notice that the head is swelling a lot, the child probably has hydrocephalus.
A surgical operation called a 'shunt' may need to be done before the pressure of the liquid in the brain causes much damage. A tube is run from a liquid-filled hollow in the brain into the entrance to the heart or into the belly (abdominal cavity). This way the extra liquid is drained from the brain.
|
|
Not all children who have early signs of hydrocephalus need this operation. If the head is not very swollen and stops increasing rapidly in size, it may get better by itself.
CAUTION: 'Shunts' do not always give good results. Even with surgery, 1 out of 5 children with hydrocephalus dies before age 7, and more than half become mentally retarded. Others are intelligent, however, and develop normally. Before deciding on the operation, get advice from 2 or 3 specialists.
| Note: We realize that, for many families, the
operations described here will not be possible. Except where
free hospital services are available, they are very costly. Before deciding on surgery, there are several things to consider:
In short, before deciding whether to operate, it is important to consider carefully how this may affect the quality of life for both the child and the family. |
Bladder and bowel management
A child with spina bifida usually does not develop the same control of peeing (bladder control) and shitting (bowel control) as other children do. The child may always dribble urine. Or, as she gets older, she may continue to empty her bladder or bowels without warning, perhaps without even knowing or feeling it. Standard methods of toilet training will not work. Do not blame or scold her for her accidents.
| WARNING: In some children with spina bifida, the
bladder does not empty completely. This is dangerous because if
urine stays in the bladder for a long time, bacteria will grow
in it and this can lead to infection of the bladder and kidneys.
In children with spina bifida, urinary infections are a frequent
cause of death.
|

A mother can learn to feel how full the bladder is, and to tap on it
gently to see if this makes the baby pee. If not, she can regularly
press gently on the bladder to push out the urine.

Later, some children can learn to empty their bladders by crying,
rolling over, laughing, or sneezing. Others learn to do it by
pressing on the stomach, like this, although this can also be risky
(see Page 209).
Some children may need to use a 'catheter' or rubber tube to get the urine out. By age 5 they can often learn to 'catheterize' themselves. (See Page 206.)

As they grow older, boys are often able to use a 'condom' connected to a bag that collects the urine. (See Page 207.)
Girls often need to empty the bladder regularly with a catheter, and perhaps use diapers (nappies) to catch any urine that drips out in between.

For girls, a mirror helps in finding the urine hole.
Most children with spina bifida can be helped to take care of both their bladder and bowel so that they stay relatively dry, clean, and healthy. Then they can go to school and do things outside the home with greater confidence. Therefore, it is extremely important that rehabilitation workers and family members help the child work out a good bladder and bowel program.
| IMPORTANT INFORMATION on urinary and bowel problems and prevention and treatment of urinary infections is in Chapter 25, Page 203 to 214. Be sure to study this chapter! |
PREVENTION and correction of contractures
Some children with spina bifida tend to develop contractures either because of muscle imbalance (see Page 78) or, less often, because of spasticity (abnormal muscle tightness). Contractures most often develop in the feet, hips, and knees. Range-of-motion and stretching exercises, as discussed in Chapter 42, can help prevent and correct early contractures.
| CAUTION: Only do stretching exercises where there
is stiffness or limited range of motion. Men joints are floppy,
do not stretch them more where they already
bend too much. For example: If the foot is stiff in this position,
do exercises to gradually bring the foot up. (See Page 383.)
But if the foot is floppy or already bends up more than normal,
avoid exercises that would stretch it even more.
|


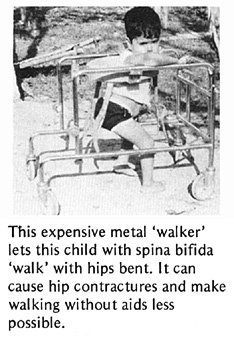
Because children with spina bifida have stronger muscles for bending than for straightening the hips, they tend to develop hip contractures, like this child.
Stretching exercises (Page 385) and lying on the belly (Page 86) may help.
Also, make sure walking aids help correct rather than increase the contractures.
Sometimes a child stands with hips and knees bent, partly because
his feet bend up too much.

This can lead to hip and knee contractures.

Lightweight below-knee braces that hold the feet in a more firm position may be all the child needs to stand straighter, walk better - and prevent contractures. (See Page 550.)
| Do not let the child get fat. Because the legs and feet of a child with spina bifida are weak, it is important that she does not get too heavy. Even for a child who does not walk, moving will be easier if she is not fat. Encourage her to eat nutritious foods, but to avoid a lot of sweets, fatty foods, and sweetened drinks. |
HELPING THE CHILD DEVELOP
Many children with Spina bifida are paralyzed from the waist down. In spite of their disability, it is important for them to develop their bodies, their minds, and their social abilities as much as possible. Certain 'adaptive aids' can be used to help paralyzed children go through the same stages of development as able-bodied children, at close to the same age. (See the developmental chart on Page 292.)
For the child to progress through the early stages of development, it is important that he can
| SEE STRAIGHT AHEAD | SIT WITH HIS HANDS FREE |
| NORMAL
|

|
| SPINA BIFIDA
|

|
| If she cannot get herself into a position where she can see what is happening in front of her, lie her on a 'wedge' or fix a carton or box so she can sit leaning back in it. | You can make a seat from an old bucket or some other object, so that she can sit and play. |
| EXPLORE HIS SURROUNDINGS | STAND WITH HIS HANDS FREE |

|

|

|

|
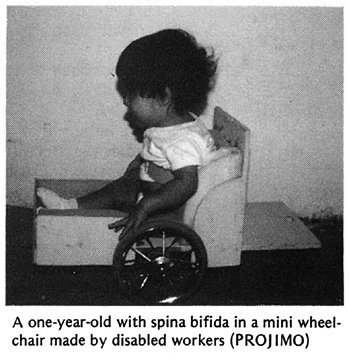
| You can make a little cart that helps her to move. The cart can have a handle so that another person can push it. | Make a standing frame that holds her in a standing position. Holding up the weight of her body on her legs will strengthen her bones, so they will not break as easily. |
| SIT, STAND, AND WALK | |

|
|

|
|
| She can use a brace that holds her up, so that she can walk with crutches. It helps if the brace has hip and knee hinges so that she can sit down (see Page 575). |


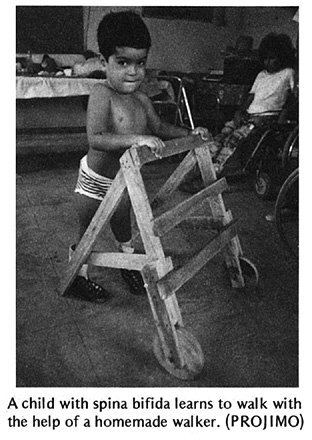
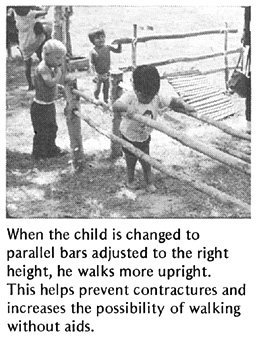
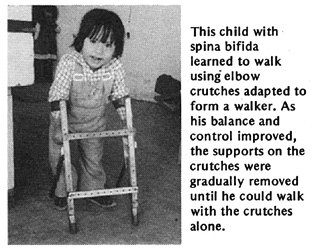
When adapting aids for children with spina bifida, remember that each child is different. Some children manage to walk without braces, perhaps with the aid of parallel bars like these, and later crutches. Others will need above-knee or below-knee braces (see Chapter 58). Other children will need wheelchairs.
Surgery and orthopedic corrections
To prevent or correct foot contractures in many children, it may be necessary to straighten the feet in the same way as for club feet (see Page 565). So that the contractures do not come back, the children will need to do exercises (see Page 115 and 383) and perhaps use simple plastic braces (Page 550), at least at night.
For curving of the spine, if severe, some children need surgery or a body brace. (See Page 164.)
For children with spina bifida who have one hip dislocated, corrective surgery is sometimes helpful. But surgery generally is not recommended for those children with both hips dislocated. Usually they will walk just as well if the hips are left dislocated - and with fewer complications and less suffering. (See "Hip Problems," Page 156.)
| CAUTION: Before any orthopedic surgery is performed on a child with spina bifida, carefully evaluate the possibility she has of walking and whether the surgery will really help her. |
PREVENTION of pressure sores and injuries
As a child who has no feeling in parts of his body grows older and heavier, there is increasing danger that pressure sores (bed sores) will form over bony areas that support his weight (mostly his butt or his feet). To prevent this:
| Have the child sleep and sit on a mattress or cushion that is soft (such as foam rubber), and move or turn over often. | |
| Examine the child's lower body daily for early signs of irritation or sores. Check especially the hips, knees, and feet. | |
| When he is a little older, the child can learn to check his own body each day for sores. |

|
| DANGER: Whether the cause is spina bifida or
leprosy, children who walk but have no feeling in their feet run
a high risk of cuts, burns, sores, and serious infections on
their feet. Teach them to check their feet every day. Also, be sure that sandals, shoes, and orthopedic braces fit well and do not cause blisters or irritation. |
|
| IMPORTANT INFORMATION on prevention and treatment of pressure sores is in Chapter 24, Page 195 to 202. Be sure to read it. Also see Chapter 26 on Leprosy, Page 223 to 225 for special footwear and ways to protect the feet. |
You will find other important information that relates to a child with spina bifida in other chapters of this book, especially:
Chapter 23, "Spinal Cord
Injury"
Chapter 24, "Pressure Sores"
Chapter 25, "Urine and Bowel
Management"
Also refer to the chapters on contractures, club feet, exercises, developmental delay, braces, wheelchairs, and special seating.