| 010
|
COMBINING THE BEST OF THE INDEPENDENT LIVING MOVEMENT AND CBR
In recent years, 2 major initiatives have evolved to help meet the needs,
defend the rights, and promote the full integration of disabled people.
These are the Independent Living movement (IL) and
Community Based Rehabilitation (CBR). Active in many countries,
both initiatives are a response to the discrimination, limited
opportunities, inadequate services, and the need for self-determination that
most disabled people experience in the world today.
The two movements have different origins. They also have
different strengths and weaknesses. IL tends to be strong
in areas where CBR is weakest, and CBR strongest in the areas where IL and
disabled people's organizations sometimes are weak.
 | Independent Living: The IL movement was started from
the bottom up by disabled people themselves. It began in the Western
industrialized countries. Through organizations like Disabled People
International (DPI), it has gradually made headway in the so-called
developing countries. IL's biggest strength is social action for
equal opportunities, led by disabled activists. Its biggest
weakness is that it is largely a middle-class movement that often leaves
out the poor. Also, living "independently" (or alone) is a very Western
value. In societies with a strong sense of community, rooted in extended
families, living "inter-dependently" (together) may be a more welcome
goal. |
| Community Based Rehabilitation: CBR, as an
international initiative, was launched by idealistic rehabilitation
experts working with the World Health Organization (WHO). Its biggest
strength is that it tries to reach all disabled people, especially
those who are poorest and in greatest need. It has an
all-inclusive plan, including both government and private initiatives.
But, too often, disabled persons still are treated as objects to be worked
upon, rather than leaders, organizers and decision makers. |
One of the biggest challenges for disability workers today is to find
ways to link the empowering self-determination of the Independent
Living Movement with the broad outreach to poor people of Community Based
Rehabilitation.
A good place to begin is by encouraging disabled persons
to take over more of the organizational and service-providing roles in CBR
programs. Where possible, disabled people's organizations can lead or advise
the programs (while making an active effort to include the poor and
voiceless). When disabled people learn to design and make assistive
equipment, and to include the user in the process, success is more likely.
| Community Based Rehabilitation (CBR)
Major STRENGTHS:
Rehab for all! Tries to reach all disabled people,
with most concern for the poor. Comprehensive plan with social focus.
Community education and involvement.
Major WEAKNESSES:
Usually organized for - not by - disabled people. Structure often
top-down. Tends to follow pre-determined recipes, rather than to seek
liberating solutions. |
Disabled Person's Organizations Independent Living (DPI,
etc.)
Major STRENGTHS:
Self-determination! Disabled people take lead in
defining their needs and demanding their rights. Goal is not to
normalize disabled persons, but to stop society's unfairness.
Major WEAKNESSES:
Because members tend to be middle class, the poor are often left out,
or their needs are misinterpreted to fit the priorities of Western
disability activists. |
|
| 011
|
TROUBLE-SHOOTING THE TIDE OF INAPPROPRIATE TECHNOLOGY
Some readers may wonder if this book is needed. Lots of manuals and
pamphlets on assistive aids and equipment already exist. They range from
high-power rehabilitation engineering to simple (sometimes overly
simplified) collections of helpful low-cost gadgets. Some of these guide
books have marvelous designs. But too often, more importance is given to
the equipment itself than to the persons who may use it. Precise steps
for construction are spelled out as if the final product were an end in
itself.
There is a need for guides that put more emphasis on
listening to disabled persons' wishes and suggestions, jointly
evaluating their needs, experimenting to improve the design of assistive
equipment, and adapting it accordingly.
The author and his co-workers have visited rehabilitation programs,
both hospital-based and community-based, in many countries. In
program after program, we see well-made, attractive rehabilitation aids
that simply do not meet users' needs. (The same is true for
exercises and therapy.) Often equipment is beautifully and skillfully
produced following detailed instructions in guide books or training
plans. But for some reason the end results do not provide the expected
benefits or satisfaction.
Not enough attention is paid to the specific needs, wishes, and
ideas of the disabled person and family members.
At worst, assistive devices and exercises become dehumanizingly
generic-ritualistic rather than functional. Around the world, two of the
most poorly fitted disability aids are parallel bars
and special seating. Here we will look briefly at
parallel bars. We look at problems with special seating in Part I.
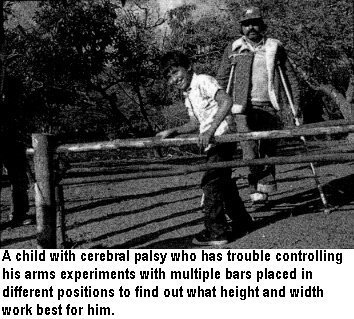
Parallel Bars: Therapy or Torture?
| Photographs or drawings of rustic parallel bars made of poles
supported by forked sticks appear on fancy brochures of major CBR
programs around the world. But on close inspection, as often as not,
the bars are inappropriate for the child using them. |
 |
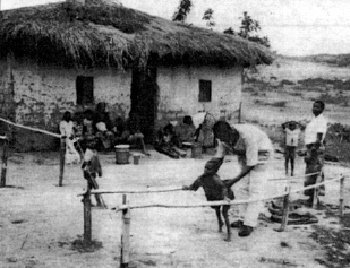 |
Here is an example from an international brochure showing a CBR
program in Burundi, Africa.(LEFT)
What problems can you see with the parallel bars used for this
child's rehabilitation?
Correct!
These bars are too high and far apart. The child, who
has weak legs, must bear most of his weight on his arms. This
requires enormous strength.
Only powerful athletes can support their full weight on
out-stretched arms, as when they perform the iron cross on
gymnastic rings. To make a child with flail legs try to do this
on bars can turn therapy into torture. |
 |
|
|
| 012 |
PARALLEL BARS should be built or
adjusted to the height and width best suited for the needs of the
individual. Usually, placing the bars fairly close together (so
the person's arms are next to her sides), at a height so her arms are
almost straight when standing upright, is the easiest and most
functional position.
Often this position creates difficulties. |
Often this position works better. |
However, depending on muscle strength of the arms and hands, and
other factors, some persons may find other positions or heights work
better. For example:
|
A child who has strong legs but lacks balance may find it easier to
walk with bars widely separated. |
A child with weak upper arms may find it easier to rest his forearms
on the bars. The bars will need to be elbow high. |
A child who tends to slump forward may find it easier to stand
straight if the bars are high, so that he has to stand upright to
rest his arms on them. |
It is essential to pay attention to the concerns of the
person who will use the equipment. Even a child who can not
speak may have ways of communicating her preferences (through tears or
smiles).
 |
 |
| It helps if bars can adjust to different heights for
different children (and to find out what height works best for an
individual child). Above are 2 easy ways. |
| Usually the best person to decide what
works best is the disabled person herself. |
|
| 013
|
The Need for Careful Evaluation of Instructional Materials
Unfortunately, photographs or drawings of assistive equipment are not
always critically evaluated before they are included in training
manuals. Likewise, many instructional materials - and training courses -
do not put enough emphasis on thoughtful, innovative participatory
problem-solving. There has been a tendency, especially in community
based programs, to deliver overly simple cookbook-like formulas for
solving the needs of disabled people. High-level decision makers often
try to find answers to the problems of marginalized people through
impersonal, standardized shortcuts (the technological quick fix) rather
than through listening and responding to the wishes of those in need. In
sum:
 |
Today there is too much doing things for
people, not enough doing things with them ... too much
giving authoritative instructions and following of recipes, and too
little creative, participatory problem-solving. Disadvantaged
persons are reduced to objects, things to be worked upon, tinkered
with, corrected, and normalized, rather than treated as unique
individuals to be empowered on their own terms. Too often the
disabled person - especially the child - is left out of the
problem-solving process. |
| There is an urgent need for training materials and
courses to place less emphasis on following standardized
instructions, and more emphasis on an observant, problem-solving
approach in which the disabled person and family members are
included and listened to as equals. |
 |
Disabled Persons and Groups Take the Lead in Designing Better
Solutions
To solve their problems, disabled people in some countries have begun
to play a leading role. Especially in the North, but increasingly in the
Third World, disabled people have organized and are demanding a say in
decisions that affect their lives. Through the Independent Living
Movement (IL), and increasingly through Disabled People International
(DPI), they insist on social rights and equal opportunity in such things
as accessibility, education, employment, and recreation. They demand a
leading voice in programs and policy-making that affect them.
In many countries, organizations of persons with disabilities have
adopted the slogan: "NOTHING ABOUT US WITHOUT US." But while disabled
activists insist on self-determination concerning social issues that
affect them, they have been slower to assume leadership in matters of
rehabilitation and technical aids. Even in the North, most disabled
persons still follow the dictates of rehabilitation professionals fairly
passively, without assuming much decision-making control. Disabled
children, especially, have almost no voice in deciding what aids or
equipment they are to use. This leads to errors in design that could be
avoided. The author himself (David Werner) as a child was given
orthopedic aids that did him more harm than good. Not until decades
later did he at last obtain appliances that worked well for him ...
thanks to a disabled village brace-maker at PROJIMO who included him as
a partner in the problem-solving process (see
Chapter 11). |
| 014
|
ADAPTING SOLUTIONS TO THE LOCAL SITUATION AND INDIVIDUAL NEEDS
Throughout the Third World you see small children in adult-sized
wheelchairs, and small thin adults in big, very wide, heavy chairs that
they can barely move.
A common shortcoming of large rehabilitation centers is that aids and
equipment tend to be standardized and "generic" (a few basic models are
intended to meet the needs of all). This is especially true when
equipment is purchased in quantity from commercial (or foreign)
producers. When standard commercial aids are prescribed, too often an
attempt is made to adapt the person to the equipment rather than the
equipment to the person.
Disabled persons' needs differ, not only individually but
also
according to local customs, living conditions and environment.
A potential advantage of a small community-based rehabilitation
center is that aids and equipment can be custom-made for each individual
as the need arises, often at remarkably low cost. Such an approach
allows greater flexibility in terms of personal preferences, as well as
adaptation to local circumstances, resources, and environment.
Four Women with Spinal-Cord Injury: Their Different Mobility
Needs
Consider for example, 4 young women, all about 20 years old, each
with a spinal-cord injury of the mid back. These are MIRA
from a village in Bangladesh; RITA from the mountains
in Mexico; LUZ from a city in the Philippines; and
FARAH from Egypt. Each, after loving support and
encouragement from family and community, got over her initial depression
and is eager to continue with life, earn a living, and take an active
part in society. But to do so, each needs an effective means of
mobility: a way to move around and go where she wants to, in spite of
paralysis of the lower half of her body.
Let us suppose that each of these young women - Mira, Rita, Luz, and
Farah - has had the luck to be given a costly imported wheelchair by an
international donor called "Wheels of Fortune." At first, all four women
were delighted with their shiny new imported wheelchairs. But within
just a few months, all stopped using them.
 Wheels
of Fortune learned that this low use-rate of donated equipment
was disturbingly common. So it sent a team of "social marketing" experts
from the North (who did not speak the local languages) to analyze the
problem. The experts concluded that "the recipients don't appreciate or
care for things given to them free." Their solution was: "Require each
recipient to pay at least part of the cost of all aids and equipment."
With such cost-sharing, the experts insisted, "recipients will
value more and take better care of the equipment they receive." Wheels
of Fortune learned that this low use-rate of donated equipment
was disturbingly common. So it sent a team of "social marketing" experts
from the North (who did not speak the local languages) to analyze the
problem. The experts concluded that "the recipients don't appreciate or
care for things given to them free." Their solution was: "Require each
recipient to pay at least part of the cost of all aids and equipment."
With such cost-sharing, the experts insisted, "recipients will
value more and take better care of the equipment they receive."
The four young women see the problem differently, If we were to ask
them to analyze and state their concerns, we might find that each has
good reasons for not using her chair. She would most likely insist that,
"If I had a chair that really helped me to move and do things
more easily, I would gladly use and care for it!" |
| 015
|
| Now let us imagine a different
scenario. Let us suppose there are community rehabilitation
workers who listen to each of the four young women and help them
figure out the best local solution to their mobility needs. Together,
they may be able to design more appropriate alternatives - liberating
solutions that free the user to lead a fuller life in her home and
community. Here we present, briefly, the stories of these 4 young
women. Though imaginary, their stories are based on reality. The
solutions they find to their specific problems within their particular
environments are based on actual innovations developed by concerned
people in different parts of the world.
MIRA, in rural Bangladesh, became
paraplegic (paralyzed from waist down) as a result of fighting between
religious groups in her village. In the hospital, a social worker gave
her a wheelchair from Wheels of Fortune. On the hospital floors, Mira
learned to move about in her chair. But on returning to her village,
she had problems. Traditionally, cooking was done at floor level on a
cooking pot called a chula. Everyone ate sitting cross-legged
on the floor. In her wheelchair, Mira was separated from her
kitchen work and from the family at mealtime. For a while she
sat in her chair without working; others served her food onto a board
across the armrests. But Mira wanted to fit in better and to
contribute more to family life. So she stopped using her wheelchair
and began dragging herself around the dirt floor on her hands and
backside. Maybe it was not the best solution, she thought. (It could
cause severe and infected pressure sores. See
Chapter 27.) But it was better than the
isolation of sitting in her wheelchair.
Solution: An answer to the needs of village women like
Mira was found at the Center for Rehabilitation of the Paralyzed
in Dhaka, Bangladesh. The Center is staffed and run mostly by
spinal-cord injured persons who seek solutions to their own and other
disabled persons' needs. They designed a "low-rider" wheelchair, or
trolley to meet village women's need to cook and eat
at ground level. First they created several working models. Then, in
response to feedback and suggestions from different spinal-cord
injured villagers, they adapted and modified the design. The trolley
can even be used as a toilet (see page 194).
Because the chair is made completely of local materials and is fairly
low-cost, it can be easily maintained at the village level. These
low-riding trollies have made it possible for women like Mira to
return to their village homes and function effectively.
| |

A metal-frame, wood-wheel trolley in Bangladesh. The rubber
tube serves as a cushion and also as a toilet seat. |

This trolley has a cushion made of coconut fiber coated with
rubber. Firm but spongy, it helps prevent pressure sores (see
p.156). |
|
|
| 016
|
RITA lives in the mountains of Mexico in a
small, pole-walled hut. She broke her lower back when she fell
carrying water from a ravine. Like Mira, Rita's fancy wheelchair is of
little use at home. She cannot ride it on the rough, narrow trails.
Her hut has 2 small rooms for 8 people. The tiny kitchen has a big mud
stove and no room to move around in a wheelchair The kitchen counter,
also made of mud, is at a height made for working standing up. And
there is no space under it to position a wheelchair. There is
simply no way for Rita to move or work effectively in her wheelchair.
Her stepmother sees Rita as useless and has begun to resent her
presence.
Solution: If after her accident, Rita's
rehabilitation workers had involved her in thinking through her
therapy and assistive equipment, they might have found more useful
alternatives. They would have realized how unsuited her environment is
for a wheelchair (especially a clumsy, oversized one).
Because her injury was low on her spine (L4), it may make more
sense to see if she can learn to walk with crutches - or at least
figure out a way to stand up to work in the kitchen. To do
this, leg braces might help: possibly simple,
lightweight ones made from plastic (see
Part 2).
To prepare for standing and walking, Rita will need an
exercise program (1) to strengthen her arms and upper body,
and (2) to maintain or increase the range of motion of her
hips and knees. If she can gradually stretch her hips and
knee joints until they bend backwards a little, she may be able to
stand and even walk (with crutches) without the need for long-leg
braces. She can do this by "locking" her legs in a back-knee position,
and by leaning her upper body backwards to stabilize her hips. She may
even be able to work standing up, with her hands free (without her
crutches).
By leaning backwards over her hips, Rita can keep her body
upright, even with no strength in her lower back. (To prevent
doubling forward, her center of gravity must be behind her hips.)
With knees bent back, she can bear weight on her weak legs. |
|

|
| Simple below-the-knee plastic braces
prevent foot-drop and help her avoid ankle-twisting on rough
paths. A slight downward angle of the foot pushes the knee back,
adding stability. |
Rocker-bottom shoes allow a
smoother gait (walking). A flat area in the middle of the shoe
soles permits greater stability for standing. |
|
With practice, Rita should be able to work standing in the
kitchen. A strap around her hips may let her work
more freely and securely. |
With effort, she may even learn to walk with crutches on the steep
trails. But she will need to develop good balance, strong
arms, and not get over-weight. |
Perhaps the best solution for travel on the steep trails will be
for Rita to learn to ride the family donkey.
|
|
| 017
|
|
Luz lives in a crowded squatter town in the Philippines.
Before her accident she worked as a health visitor,
checking the weight of young children in their homes and giving
nutritional advice to mothers. After her accident, she found
that her new imported wheelchair was too wide for narrow
pathways or to fit through the very narrow doorways of many of
the shacks. |
 |
 |
Solution: Fortunately, a program
run by disabled persons called House With No Stairs
(see page 342), has for years
been experimenting with innovative designs of lightweight,
low-cost wheelchairs. One of these has a horizontal folding
mechanism (rather than a vertical "X"). This allows the user to
easily make the chair narrower while riding it.*
________________________
* This innovation for pulling the wheels in close to the body
in order to pass through narrow doorways has been further
developed by Ralf Hotchkiss, a paraplegic wheelchair designer
who has spent years teaching disabled groups to make and design
locally appropriate wheelchairs. Among many others, Ralf has
worked with the House With No Stairs wheelchair
building team in the Philippines. For more discussion about this
and Ralf's many wheelchair innovations, see
Chapter 30. |
So after they discussed Luz's needs with her, the workers took
her measurements and went to work building her a wheelchair
with adjustable width.
 |
For ordinary use, Luz uses her wheelchair at its normal
width.(Left) When she comes to a narrow doorway, she pushes
her chair's wheels close against her hips, and passes
through.(Right)
Then she opens the chair again to its more comfortable
width.(Left)
Thanks to a wheelchair that was designed to help her overcome
the barrier of narrow doorways, Luz was able to continue her
work and earn a living helping other people.
|
 |
|
| 018
|
FARAH lives in the Egyptian
desert.
Since her accident she has joined a women's cooperative where she
can make clothing on a sewing machine, and sell it in local stores.
But the cooperative is in another village, about 2 miles away on a
sandy, rocky road. The narrow wheels of her imported wheelchair sink
into the sand, making travel impossible.
| Solution: Farah described her
frustration with getting stuck in the sand and rocks to the
local community based rehabilitation team. Together they tried
to come up with a solution. They thought of putting extra wide
bicycle tires on the wheelchair, so it would not sink in the
sand. But they could not find tires that matched the wheels of
her chair. So they made a new, simple wheelchair using wide
bicycle wheels. For the small front wheels they used thick disks
made with several layers of plywood, covered with a wide strip
of car tire. When Farah tried her new chair, the small front
tires sunk somewhat less in the sand. But they got caught easily
on small rocks. The wheelchair stopped so suddenly that
sometimes Farah was almost thrown out ,of her chair. |
 |
Farah suggested bigger front wheels. But the CBR team pointed out
that if the front castor wheels were larger, they would bump into
the footrests on making a turn. What to do?
 |
One of the CBR workers remembered a picture he had seen of a
"tricycle wheelchair" with a single large front wheel, mounted
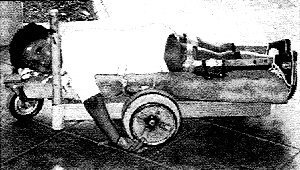
in front of the footrests. So the team built a "trike" for Farah
using extra wide bicycle tires on all 3 large wheels,*
_______________________
* There are many designs for tricycle wheelchairs, powered by
one or two hands.
See Chapter 31.The trike, powered
by a hand lever, was a great success. Farah found it ran well on
the sand and gravel roads. She could make it move so fast that
it sailed through soft patches of sand without slowing down or
getting stuck. She loved it! |
In conclusion ... The 4 young women - Mira, Rita, Luz,
and Farah - all found different solutions to their different local
and personal needs. This was possible because local rehabilitation
workers listened to the women and involved them in planning and
testing various innovations and adaptations. For 3 of the women, the
solutions involved specially designed wheelchairs. But for Rita -
who lived where wheelchair mobility was virtually impossible - it
meant learning to stand and walk with braces, and riding the family
donkey.
|
| 019
|
Examples from Real Life
While the stories of the four women with their
different wheelchair needs are imaginary, they are based
on experiences of real women. "Low-rider" wheelchairs or
"trollies," such as the one adapted for Mira's needs,
are produced for paraplegic women in Bangladesh by the
Center for Rehabilitation of the Paralyzed.

This woman in Bangladesh uses a trolley in her home
business, raising chicken and selling eggs. Having an
income of her own increases her independence and wins
her community's respect. Photo by Shahidul Haque for
Social Assistance and Rehabilitation for the Physically
Vulnerable (SARPV).
Wheeled cots can also be adapted to local
customs.
|
|
|
| In most countries, trollies (wheeled cots or
gurneys) are at a height so the person can eat and
work at a table. This boy is on a gurney in order to
remain active while his hip and knee contractures
are straightened. (For more on gurneys and trollies,
see Chapter 37.) |
This floor-level trolley, or wheeled cot, was
developed by the same program in Bangladesh that
builds low-rider wheelchairs. It allows this boy to
join his family for meals on the floor. (The boy
needs to lie on his belly to heal pressure sores on
his backside and to correct his hip contractures.) |
|
|